PCOS Guide + Protocol
PCOS isn’t just hormonal - it starts with disrupted patterns of energy, timing, signalling, and trauma. This is everything you need to know.

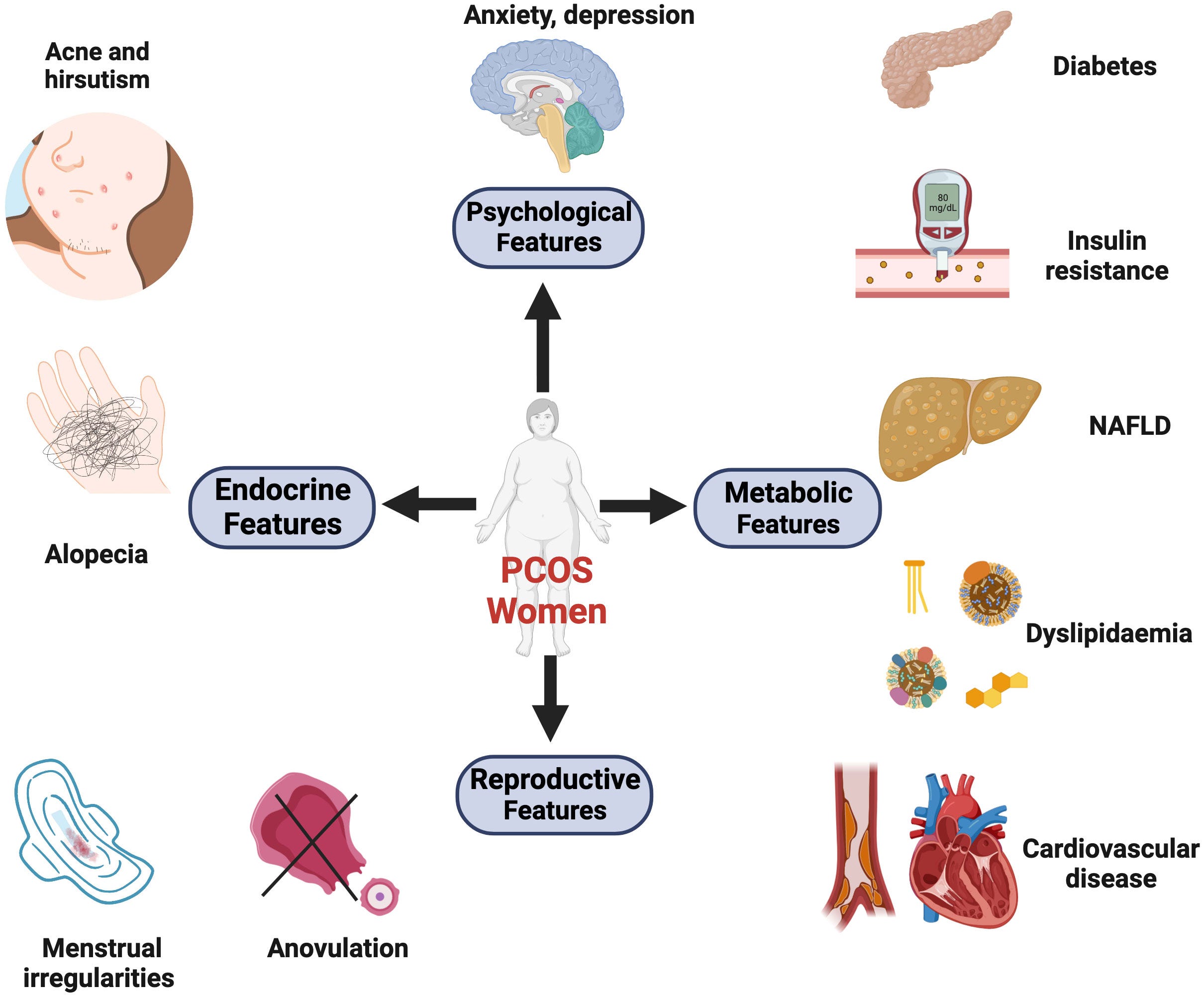
Polycystic Ovary Syndrome (PCOS) is a common hormonal disorder affecting women, characterized by irregular periods, excess androgens, and/or polycystic ovaries.
It affects about 1 in 10 women of reproductive age, and can lead to a range of symptoms including irregular or missed periods, excess facial or body hair (hirsutism), acne, and difficulty conceiving. PCOS can also increase the risk of developing type 2 diabetes, heart disease, and other health problems.
It’s also important to note that up to 70% of women with PCOS may have unrecognized endometriosis - see my protocol for that HERE.
…and 80% of menstrual blood in endometriosis contains lipopolysaccharide (LPS), an endotoxin derived from negative-gram bacteria due to gut dysbiosis.
This is not a diagnosis to be managed - it is a call to reset the system. A deep one that includes light environment, mitochondria/bioenergetics, nervous system, toxins/heavy metals, gut health, hormone balancing, metabolic health, and trauma. This guide is the blueprint for that reset.
PCOS is to women what male pattern baldness is to men - not a disease of excess testosterone, but a sign of localized androgen dominance happening inside a dysregulated, energy-poor system. In both cases, it’s not that androgens are the enemy, but more so the local terrain that’s disrupted - energy, timing, and signalling is awry.
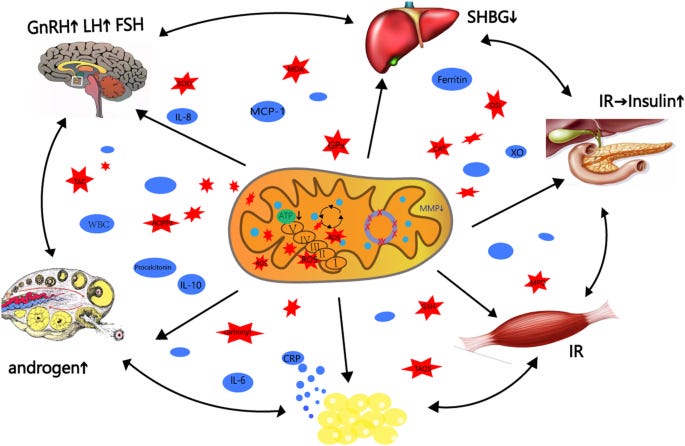
Poor mitochondrial function, disrupted circadian signals, chronic inflammation, and immune stress create an environment where androgens act destructively instead of regeneratively. Balance is key when it comes to hormones, as their signals of our environment. PCOS is a miscommunication between hormones, light, metabolism, gut, and the brain-ovary axis. It’s the female version of a deeper systemic misfire.
You don’t always need an ultrasound to suspect PCOS - blood work reveals the internal chaos before it becomes structural. If you know what to look for, you can often catch it early, long before cysts form or periods disappear:
Fasting insulin over 6 uIU/mL and glucose above 90 mg/dL, or an HbA1c creeping past 5.4 - these are signals of early insulin resistance, one of the metabolic roots of PCOS.
An LH to FSH ratio greater than 2:1 often reflects hypothalamic mis-signalling, with GnRH firing too frequently and pushing androgenic pathways
SHBG under 40 nmol/L means more free testosterone is circulating and causing localized issues - acne, hair growth, and menstrual disruption often follow
Free testosterone over 15 pmol/L can appear even when total testosterone looks normal - always look at free T and SHBG
Progesterone low in the luteal phase (days 21-23) - often <5 ng/mL, or a PROG:E2 ratio skewed far from 1:10 to 1:15, reflects poor ovulation and menstrual regulation
Estradiol might be high, low, or erratic depending on the subtype - what matters is the ratio between it, PROG, and TEST - and its recycling via the gut (WBCs + bilirubin + liver enzymes will give clues)
Look at markers of liver detox - elevated ALT/AST or GGT suggests a sluggish phase I/II system, which matters for hormone clearance
If available, DUTCH testing may show elevated androgens/DHEA, estrogen metabolites, low progesterone, and overall hormonal imbalances
DHEA-s elevation points toward adrenal hyperactivity, often from chronic stress or trauma - context is needed.
High hs-CRP and/or ferritin via IL-6/inflammation/LPS might signal ongoing low-grade inflammation that’s driving insulin resistance
If you have access to zonulin on a GI map - elevation reflects gut permeability, a major trigger in many women with PCOS
Now, this is everything you need to know, and everything you need to do.
Chakra Blockades, Trauma, & Nervous System Dysregulation //
This is by far one of the most interesting connections when it comes to PCOS.