

How ALL DISEASES Begin & End with OXYGEN
ALL diseases are controlled by this mechanism and this is WHY you should pay attention.

I just recorded a podcast yesterday that touches on this very topic that you should all listen to in a couple of weeks.
You can spend years chasing symptoms across systems and still miss the one place where the story always starts and ends.
The way you, your family, or your client’s mitochondria reduce oxygen at cytochrome c oxidase (CCO) - the terminal enzyme of the electron transport chain (ETC), decides whether physiology stays coherent or slides into entropy.
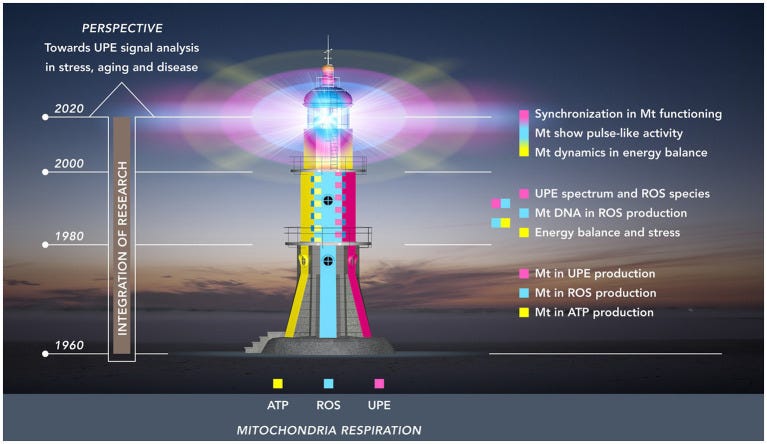
When oxygen is matched to electrons and protons cleanly at complex IV, water forms, redox improves, ultra-weak photon emission settles into order, and the organism expresses resilience.
When that coupling stutters, the organism compensates by downgrading hardware, leaking light, and reprogramming metabolism toward survival at the cost of function. What follows is a practical, detailed way to see the whole thing at once, so you can intervene where it actually counts.
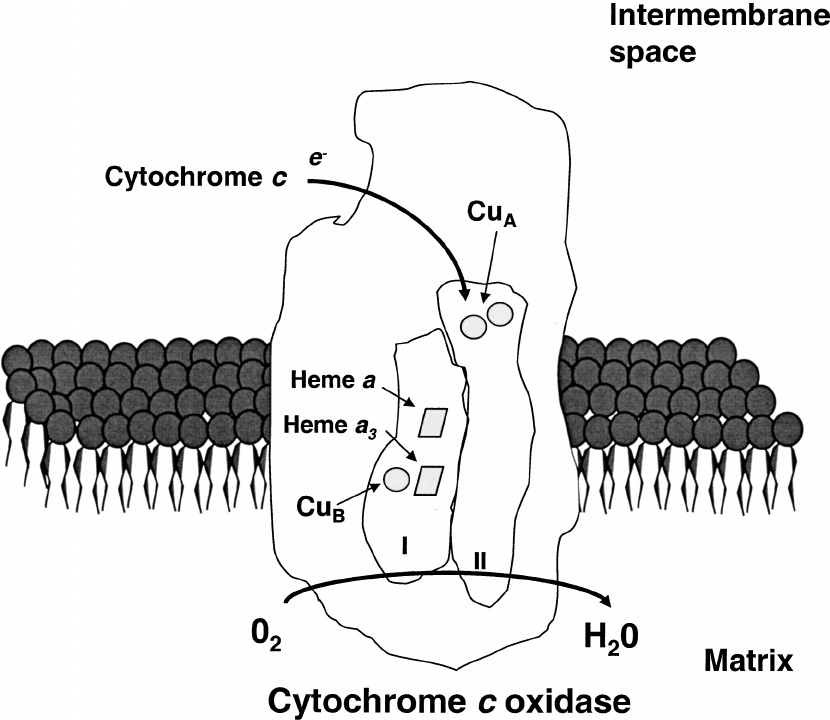
The overall reaction formula for cytochrome c oxidase is the four-electron reduction of oxygen to water: 4Cyt cred + 4H+ + O2 → 4Cyt cox + 2H2O.
CCO also requires transition metals - Heme Iron and Copper - to function correctly. These transition metals act as redox centers for electron transfer and oxygen binding. Their unpaired d-electrons make them exquisitely sensitive to weak magnetic and electric fields. In the geomagnetic field of the Earth, their spin states and redox cycling remain optimally tuned, but artificial EMFs disrupt this balance through radical pair mechanisms. This is not limited to Iron and Copper, but also any enzymes that utilize Cobalt (B12), Manganese, Zinc, Magnesium, Nickel, and Molybdenum.
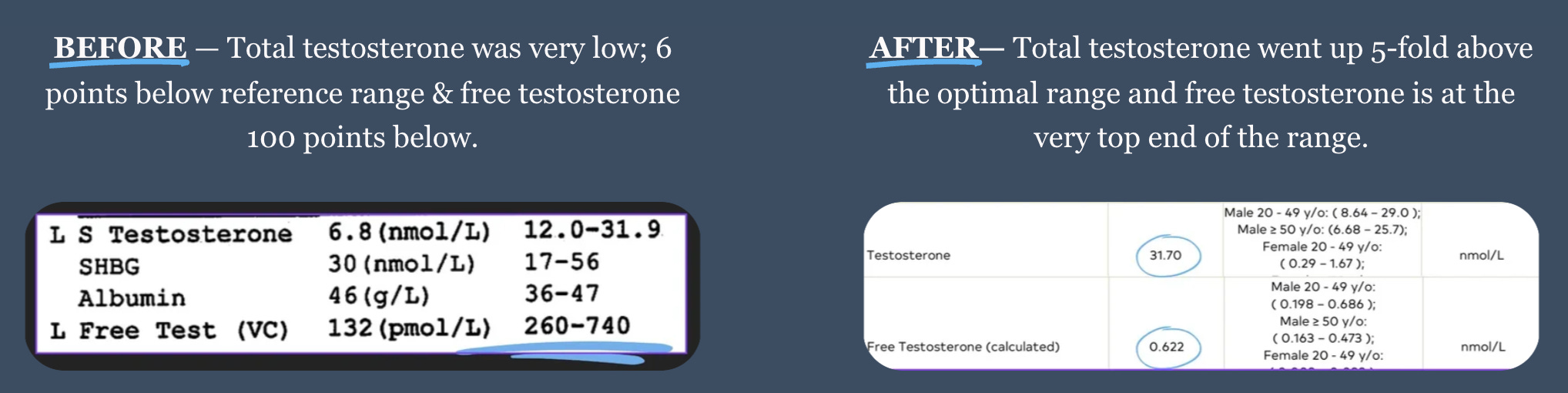
I learned this the long way around: Years back, in the middle of chronic stress, buried trauma, blue light nights, drugs/alcohol, processed food, pornography, and an addiction to scrolling - my testosterone fell below the range, my sleep fell apart, and my nervous system lived on sympathetic fuel.
Endocrinology labs did not explain why. Diet flips helped a little. What changed everything was moving my life outdoors and rebuilding light, magnetism, and electrons as first inputs, because that is how you change oxygen use at the mitochondrial level.
The more I studied and coached, the clearer the pattern became. When you rebuild the conditions that let oxygen be reduced at complex IV cleanly and rhythmically, you do not just normalize a lab, you turn the system back into a coherent, information-rich field.
The Core Problem: Oxygen, Stress, & Hypoxia //
ALL chronic conditions and diseases carries a signature of poor oxygen use that you can trace right down to complex IV. Cytochrome c oxidase (CCO) accepts electrons from cytochrome c, matches them with protons, and reduces oxygen to water, which pushes the gradient that drives ATP synthesis.
This is not an abstract idea, it is the fulcrum of life’s energy economy, and any persistent mismatch between oxygen supply, electron flow, and proton recycling shows up as falling ATP, sporadic endogenous light patterns, rising reactive species without timing, swollen water networks, and a drift toward defensive metabolism.
The literature is clear that CCO is the terminal oxidase completing oxygen reduction in oxidative phosphorylation. Many researchers also treat it as the primary intracellular photoacceptor for therapeutic red and near infrared light, while others argue that bound water at the enzyme is a dominant target, so your mental model should hold both possibilities without losing the clinical point, which is that this site governs the fate of oxygen and therefore governs function. It's also important to note that oxygen absorbs IR light itself too. These are your first clues.
Stress, in practice, is simply every input that drives hypoxia signalling.
A person's external light environment, their emotional load, their toxicants, their sleep apnea, their biomechanics, and their training context all converge on the same molecular switch.
As oxygen tension falls, HIF-1α stabilizes, and transcription shifts the cell away from oxidative phosphorylation toward glycolysis, glycogen synthesis, and glutamine rerouting for lipids.
That shift buys time, but it is a downgrade in information density and energetic coherence, and if it persists the organism behaves like a grid under intentional electrical brownouts, where noncritical lines are cut to preserve the core.
The fascia tightens, perfusion changes, and local fields lose their rhythm. This is how you end up palpating a neck that feels like it needs a weekly massage just to keep the lights on.
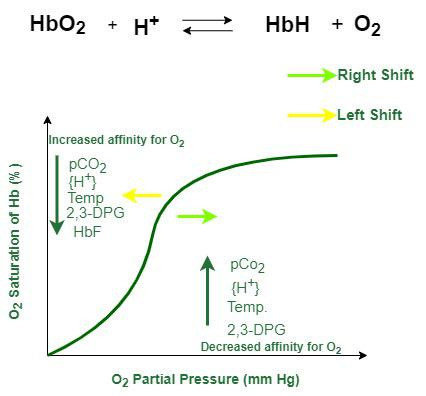
The blood side of the story is not only about oxygen content, it is about delivery. Hemoglobin must let go.
Carbon dioxide and pH modulate that unloading through the Bohr effect, which means chronic overbreathing, shallow chest patterns, or mouth-open sleep that dumps CO₂ will starve tissues that appear well oxygenated on paper.
You cannot read PaO₂ and assume utilization is fine if CO₂ handling, posture, or airway mechanics are compromised.
This is why addressing sleep apnea, biomechanics, fascia, ribcage shape, nasal resistance, and diaphragmatic strength often moves the needle on fatigue, brain fog, and libido more than yet another supplement.
Nitric oxide adds another layer, since NO binds to and reversibly inhibits cytochrome c oxidase in competition with oxygen.
In small, paced pulses NO regulates mitochondrial respiration (iNOS) and signaling. In stressed tissue with mis-timed NO or nitrite pools, inhibition of CCO can become a brake that the system rides constantly, which looks like fatigue, cold hands, slow cognition, and a low ceiling for work.
The nuance for you is that light can change this dynamic because the heme-copper binuclear center and neighboring chromophores respond to red and near infrared, and some authors propose that photobiomodulation can modulate NO binding, nitrite reduction, and oxygen kinetics at the enzyme.
Clinically, this is why sunlight or targeted NIR often feels like it “opens” metabolism in cold, dull tissue without pushing stimulants.
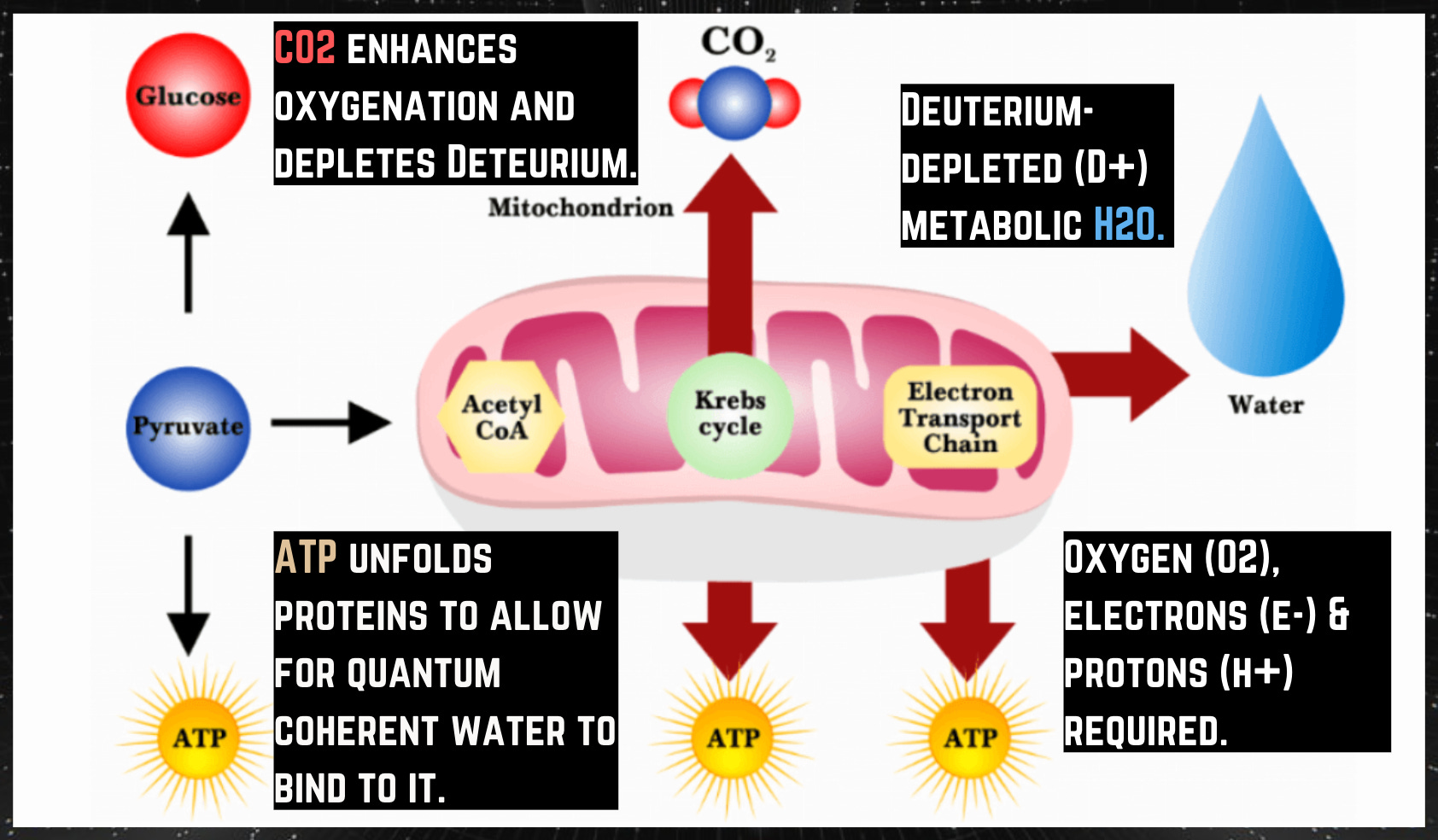
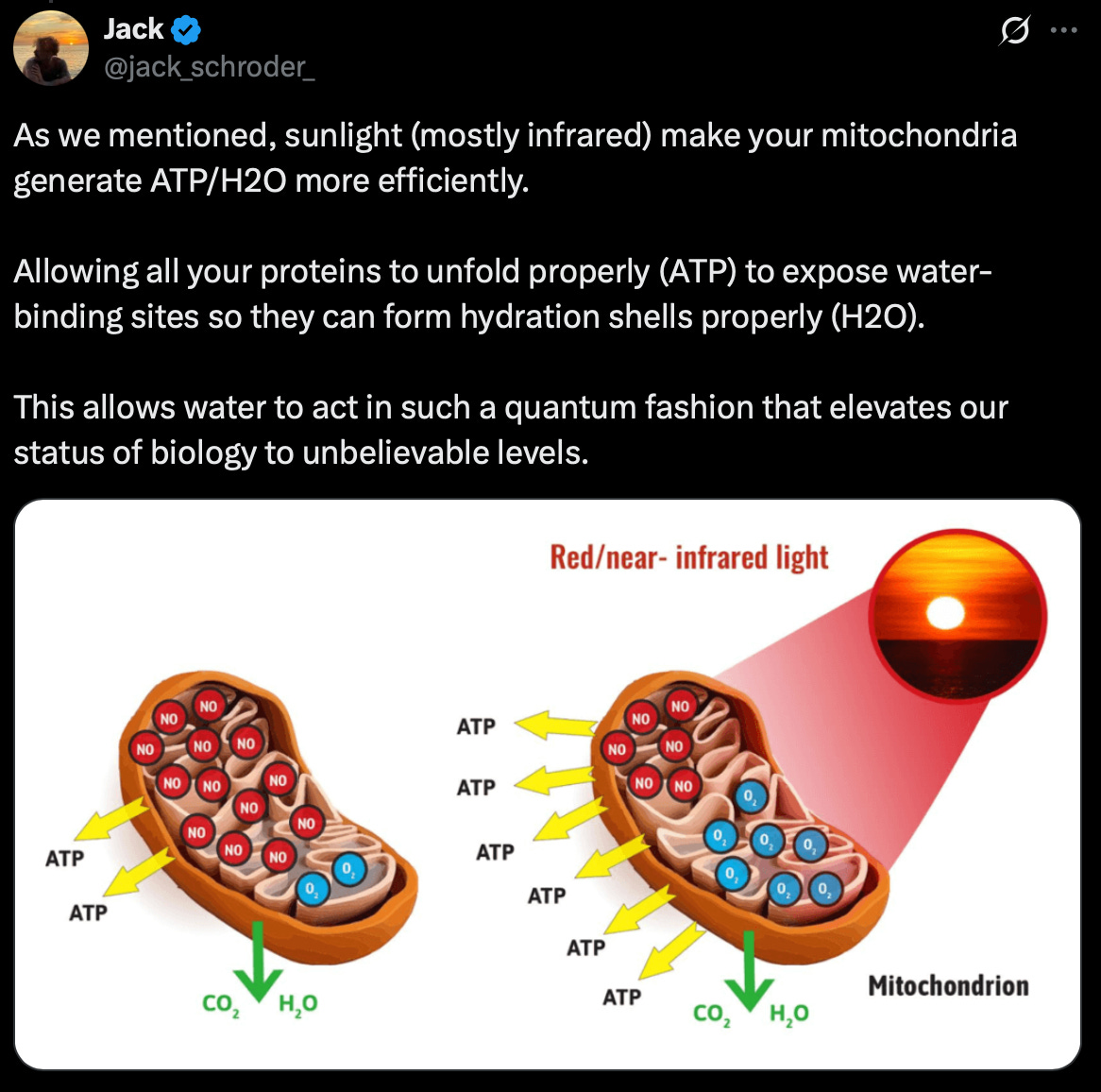
To really oxygenate tissues - to run your mitochondrial engines at full capacity to make ATP + H2O + UPEs - there’s a dance between oxygen (O₂), nitric oxide (NO), and carbon dioxide (CO₂). Each is just as important as the other.
O₂ absorbs infrared light from the sun/UPEs, forms singlet oxygen, and binds to hemoglobin (Fe²⁺).
NO is made via eNOS with UVA light, driving vasodilation and microvascular flow.
CO₂ is generated by mitochondria and retained with proper breathing mechanics, enabling the Bohr effect - the actual release of oxygen into tissues.
When a client lives in chronic hypoxia signals, the body protects itself by downgrading semiconductors and transport lines - a downgrade of bioelectrical infrastructure. Collagen dehydrates and loses conductivity, melanin density falls, myelin function drops, DHA-rich membranes stiffen, and microtubule water networks becomes noisy. The organism is saving itself from combustion by making itself less able to burn (oxygen, protons, and electrons), which looks like neurlogical disorders, heart disease, gut dysbiosis, weight gain, insulin resistance, and brain fog for the person, and looks like a translucent, low-signal body to anyone who can see the physics.
Scan for this pattern in intakes:
Lack of sunlight, grounding, and nature - missing infrared, ultraviolet, and magnetic inputs, lowered electron flow, degraded melanin, low melatonin, GABA/glutamate, dopamine imbalance, chronic inflammation, nervous system noise
Blue light exposure - screens, LEDs without balanced sunlight → circadian redox mismatch, melatonin suppression, hormone drift
Gym training indoors - artificial light, poor air, no ground contact → hypoxic training, low recovery, poor gains
Airway issues - mouth breathing, snoring, apnea, narrow palate, forward head posture → low CO₂, poor oxygen unloading, nervous system strain
Chronic emotional load - fear, news cycles, isolation from nature → sympathetic dominance, HIF-1 signaling, inflammatory drift
Processed food - proxy for low redox and missing natural EMF/light inputs → over-reliance on food electrons, gut inflammation, immune dysregulation
Tie into broader assessment:
Cross-system symptoms - gut, hormones, mood, immune all echo the same oxygen deficit
Health history - heteroplasmy load shows up in siblings, parents, grandparents; family illness = shared mitochondrial fragility
Developmental roots - neural crest migration (weeks 2–16) sets up neurons, glia, melanocytes, gut enterochromaffin cells, osteocytes; disruptions here = lifelong vulnerability under stress
You are not looking for a single cause. You are mapping a consistent drift toward hypoxia signalling that ends at complex IV.
This is just Section One, we have got plenty more to dive into - and how to optimize this for yourself, your family, and your clients.